2019 Gastrointestinal Meetings at a Glance
The current COVID-19 situation means businesses are not running as usual, rendering prospective conferences being put on-hold. Whilst many of us have looked forward to our annual presentations and reunions with colleagues in 2020, we may realistically be looking at convening through some form of digital platforms instead, if not to be stalled for later date. For those who managed to make it for some of the 2019 colorectal conferences, one may agree that it had been one fruitful year with GI and Colorectal Surgery. I have put together a summary of a few conferences in 2019 (leaving out the main stream BAPS / EUPSA) to offer food for thought and mind stimulation, although by no means exhaustive. Please feel free to put your comments through for discussion.
9th UKPCG Meeting, Oxford, Jan 2019

-
- We started off with the preliminary report on NET2HD study, looking at the outcome of Hirschsprung’s in the UK based on the BAPS-CASS cohort recruited over a 2-year period in 2010-2012, and followed up until the age of 5-7 years. Based on 177 patients with completed data, Soave (55%) and Duhamel (35%) procedures predominated. Fecal incontinence based on its definition of ‘involuntary passage of faecal matter in an inappropriate place’ was ~60%, with ~20% needing enema or washout. As a result half of these patients had PedsQL score of over 1SD below mean.
- Data from Oxford highlighted the risk of urinary tract dysfunction following PSARP. A pre-emptive suprapubic catheter could be worth a consideration. A systematic review from London was presented reviewing risk factors for lower urinary tract dysfunction in ARM. It highlighted the nature of anorectal malformation being a disease inherently associated with a risk for neuropathic bladder due to spinosacral anomaly, and high incidence of renal tract abnormality, compounded by potential intraoperative pelvic nerve injury with dissection of common wall between urethra and rectum. Urodynamic assessments had been proposed before and after PSARP.
- We heard about the Norwegian experience in deepening understanding of Transition Care through qualitative research conducted systematically through focused group discussion in adults aged >18 years, followed by analysis through an inductive process to put issues into ‘themes’. This identified somatic and psychological challenges that better prepare our teenage patients for transitioning, and offering appropriate support. For surgeons, it means having a truly long term follow-up, assess needs during transition, and identifying key adult services that can appropriately look after patients with major colorectal reconstruction.
- Two talks on rectal prolapse were given by adult and paediatric surgeons brought our attention to NICE guideline 2018 [IPG618] on laparoscopic ventral mesh rectopexy. Surgeons performing this procedure needs to take appropriate steps to ensure safety, complications, and efficacy are considered and discussed with pelvic floor MDT and parents / patients.
- Experiences of pouch surgery in IBD from Bristol and Newcastle strengthened the argument for having adequate volume to develop expertise, which can be acquired through joint surgery with adult colorectal surgeons in high volume centres. Having a dedicated service, with regular audit put in place to ensure outcome is constantly evaluated could not be overemphasised.
BSPGHAN, Oxford, Jan 2019
-
- Summary on the 5th UK Complex Nutrition and Intestinal Failure Network Meeting:
- Complication of jejunal feeding, a well-known problem, especially with gastrojejunal tubes, urging the need for clear indication before initiating jejunal feeding, and having a de-escalation strategy put in place.
- Blenderised diet through feeding tube, which currently lacks research data on nutritional value and efficacy, carries risk of tube blockage, yet recognised as a potential for cost-saving, should be the focus for future research.
- Central line associated bacterial infection (CLABSI) – Ethanol line block has been shown to reduce line sepsis by 63% in a meta-analysis (Rahhal et al. JPEN 2018), acknowledging that it is used more in USA than the UK. Taurolidine line lock (Taurolock™) has also been affirmed in 3 studies, including one from GOSH (JPGN 2012) to be effective in reducing CLABSI.
- Summary on the 5th UK Complex Nutrition and Intestinal Failure Network Meeting:

-
- Novel therapy in constipation – the use of prucalopride (selective 5HT4 receptor agonist) and lubiprostone (intestinal chloride channel activator) has been licenced and shown to work in adults, but remain under-utilised in children due to limited trials and none showing clear benefit. Other new agents include linaclotide, plecanatide, elbixibat, and tenapanor are agents yet to be tested. It is acknowledged that treatment efficacy for constipation is more difficult to be demonstrated in children because it remains more heterogenous with associated fecal incontinence, less likely to be slow transit than in adults, and the improvement in placebo arm of trials were more pronounced.
- A really useful talk regarding safeguarding children with constipation (or multiple food intolerances) as primary symptom. Two take-home messages: (1) consideration to refer to social services if there are indicators for neglect (‘not brought’, non-compliance) or fabricated or induced illness (https://www.nhs.uk/conditions/fabricated-or-induced-illness/symptoms/); and (2) beware of medical child abuse, i.e. when fabricated or induced illness had led to medical staff believe what parents reported, and resulting in harm. An MDT approach should be considered prior to any major surgical undertaking.

- Professor Russell Viner, President of RCPCH, talked about the unmet needs of adolescents. He stressed the importance of recognising the prolonged adolescence stage (up to 24 years) when dealing with chronic disorders, despite hospital set-up simplistically dictates 16 years old being the point of transition into adult services. Considering 29% of adolescents with long term condition have mental health disorders, he drew our attention to an old DoH document that showed reduced death, unplanned admission and A&E attendance if good adolescent care is provided, whatever the setting is. (https://dera.ioe.ac.uk/8742/2/A9R93BB_Redacted.pdf)

Advanced Coloproctology Course, Sheffield, Apr 2019
ACPGBI runs this course yearly to discuss key topics on coloproctology. I selected a few updates that may be relevant to paediatric practices:
- Proctology – I will spare you anodermal skin conditions and haemorrhoids which are primarily adult diseases. In the world of fistula surgery, however, much has developed beyond the standard laying open of fistula which is common practice in very young children due to their low-lying infrasphincteric nature. The surgeon’s role in sepsis drainage (I&D, seton, usually not laying open) followed by medical therapy (steroid, thiopurine, and biologics) is the general rule in managing complex fistula-in-ano, particularly those with perianal Crohn’s disease. Although multimodal therapy involving a gastroenterologist is key to optimal treatment, long-term studies from Netherland (Molendijk 2014) depressingly showed that the remission rate of complex fistula is still only 37%. Emerging sphincter preserving surgeries (e.g. VAAFT, OTSC, FiLaC) provides alternative modalities of treatment beyond the use of seton, but good evidence about efficacy, even in adults, is limited. Adipose-derived stem cell therapy appears to offer benefit in achieving short-term fistula closure in one RCT (Panés J et al. Gastroenterology 2018) but it is an expensive treatment which is available in limited specialist centres.
- Emergency – The adult emergency bowel surgery data were presented through two major audits – NELA (National Emergency Laparotomy Audit, since 2013, latest report here , and NASBO (National Audit of Small Bowel Obstruction, in 2015-2016, report from 2017 here https://www.acpgbi.org.uk//content/uploads/2017/12/NASBO-REPORT-2017.pdf).
- The quality of care for children’s abdominal surgery is currently being audited prospectively through CASAP (Children’s Acute Surgical Abdomen Programme, https://www.niaa-hsrc.org.uk/CASAP-Home) run jointly between BAPS and Association of Paediatric Anaesthetics, so do talk to your local PI about how to take part.
- Sepsis –The Surviving Sepsis campaign guideline (2004) that initiated early goal directed therapy (EGDT) had evolved through time, with endorsement by UK Sepsis Trust (and NICE) to produce a simplified guideline (Sepsis-6) to help junior doctors practise evidence-based management both in term of sepsis recognition, and early management.
26th Paediatric International Colorectal Club Meeting, Serbia, Jun 2019

- Tomas Wester (Stockholm) gave one of the keynote lectures on the association of inflammatory bowel disease (IBD) with Hirschsprung’s disease (HD). He provided compelling evidences using the Swedish National Patient Register over 50 years to identify patients with IBD and HD which found the odds ratio for IBD = 5 in HD, compared to control (Löf Granström et al. JPGN 2018). Crohn’s disease being more associated than ulcerative colitis. Hirschsprung’s associated enterocolitis could be a potential risk factor for IBD, based on alterations in microbiome, serological markers (increased IgA ASCA, OmpC), and fecal short chain fatty acids.
-
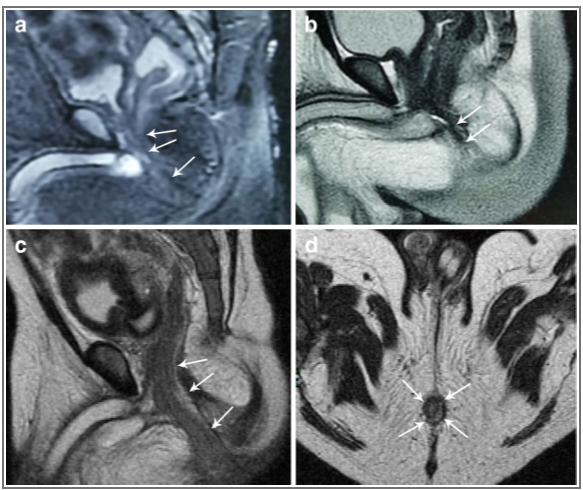
- Long Li (Beijing) presented a large series laparoscopic assisted anorectoplasty (LAARP, n=330). This had since been published (Li et al. PSI 2020). The technique challenged the standard Pena’s PSARP approach, especially given its excellent functional outcome.
| a Before laparoscopic assisted anorectoplasty (LAARP), MRI visualizes the longitudinal muscle tube (arrows) in the patient with a prostatic fistula, b before LAARP, MRI visualizes the longitudinal muscle tube (arrows) in the patient with a bulbar fistula. c After LAARP, MRI visualizes the rectum located in the longitudinal muscle tube for the patient with a rectoprostatic fistula (sagittal image), d after LAARP, MRI visualizes the rectum located in the longitudinal muscle tube for the patient with the rectoprostatic fistula (coronal image)
Li L, et al. Pediatric Surgery International 2020;36:279-287 |
Strategies and Trends in European Pediatric Surgery (STEPS) – Complications in Paediatric Colorectal Surgery, Ankara, Oct 2019
This great expert forum covered a broad range of topics reviewed by an international faculty.
- Enterostomy problems were reviewed at length, pointing towards higher complications related to NEC and IBD. Other factors including on/off laparotomy wound and loop/end stoma do not appear to make significant difference. Timing of stoma closure in NEC remains controversial despite meta-analysis of 6 studies showed no difference in outcomes and complications between early and late (>8weeks) closure (Zani et al. EJPS 2017).
- Hirschsprung’s disease and motility disorders
-
- Transanal endorectal pull through (TERPT) was extensively discussed. Since its first description (De La Torre-Mondragon et al., JPS 1998), its proponents claim expediancy, no adhesions, reduced blood loss, cost saving, and being ‘scarless’. The argument of cuff – long or short, (Soave) or no cuff (Swenson) remain unresolved. Several valid concerns had been raised nonetheless. Did it cause extensive anal stretching and sphincteric damage (and higher incontinence)? Would it work for long segment or total colonic HD? Was it beneficial having a transabdominal rather than a complete transanal approach? The evidences offered appear to dismiss many of these arguments (or at least demonstrated achievability) – manometry evidence of post-TERPT showed little change (Till et al. EJPS 2006), with short and long term functional outcome studies from Scandinavia (Stensrud et al. JPS 2010; Neuvonen et al. Ann Surg 2017) and Japan (Onishi et al. JPS 2016) demonstrating comparable outcomes with abdominal approach. A recent meta-analysis (Yan et al. Medicine 2019) concluded that TERPT is superior to transabdominal approach in terms of hospital stay, postoperative incontinence, and constipation.

- The issue of which technique to choose, as summarised by Jean-Michel Guys, is much a matter of which potential complications you wish to manage: Soave (cuff too tight), Duhamel (rectum too long), Swenson (anastomosis too high and increasing with age). As always, the 3 basic rules of HD surgery had been emphasised – absorbable suture, tension free anastomosis, and maintaining good vascularisation.
- The unique series of Variant HD from Dublin was presented. Although there are a few differential diagnoses related to childhood intestinal dysmotility which resemble HD, in the presence of ganglion cells, an algorithm of diagnostic work-up is useful to determine: intestinal neuronal dysplasia (IND), intestinal ganglioneuromatosis, isolated hypoganglionosis, immature ganglia, absence of the argyrophil plexus, internal anal sphincter achalasia (IASA) and congenital smooth muscle cell disorders such as megacystis microcolon intestinal hypoperistalsis syndrome (MMIHS) (details are in Friedmacher and Puri, PSI 2013;29:855-872)
-
- Anorectal Malformation
- The group from Tokyo presented a series of laparoscopic versus posterior sagittal anorectoplasty (LAARP n=26 vs. PSARP n=19) which highlighted the better outcome in the LAARP using a range of objective measurements – magnetic resonance image score (MRIS), fecal continence evaluation score (FCES), anorectal angle with barium enema, and surgical stress (Yazaki, Koga et al. PSI 2016). The conclusion was: LAARP was more favourable because MRI showed comparable symmetrical reconstruction compared to PSARP, but LAARP had less analgesia requirement and consistently better FCES.
- In regards to avoid anal stricture/stenosis, traditional ‘anal flap’ concept has been brought forward for discussion again, to challenge the typical circular coloanal anastomosis. Nixon triangle, Mollard flap, or Mollard-Pena (MOPE) procedure are in theory more ‘physiological’ as an anal canal (for sensation) and cosmetic.
- The Columbus, OH, experience in managing various complications were discussed, and many have already been well published.
- Of the 153 redo-PSARP, mislocation (61%) and stricture (36%) were the commonest indications. The 1-year follow-up laxative requirement was 49% and, for those who were potty trained, continence was 76%.
- Skin level stricture managed with Heineke-Mikulicz anoplasty has been published in Halleran et al. JPS 2019
- Remnant of original fistula (ROOF), for which 87.5% needed a redo, has been published in Rentea et al. JPS 2019
- Cloaca
Two up-to-date and comprehensive talks on cloaca surgery summarised the recent studies that had helped surgical planning (Columbus), and reported long term outcomes (Helsinki). These publications are summarised as follow:
- Rintala R. Congenital cloaca: long term follow-up results with emphasis on outcomes beyond childhood. Sem Ped Surg 2016;25:112-116
- Reck-Burneo CA, et al. The use of rotational fluoroscopy and 3-D reconstruction in the diagnosis and surgical planning for complex cloacal malformation. JPS 2019;54:1590-1594
- Gasior A, et al. Transcending Dimensions: a Comparative Analysis of Cloaca Imaging in Advancing the Surgeon’s Understanding of Complex Anatomy. J Digit Imaging 2019;32:761-765
- Halleran DR, et al. Urethral length in female infants and its relevance in the repair of cloaca. JPS 2019;54:303-306
- Wood R, et al. Cloaca reconstruction: a new algorithm which considers the role of urethral length in determining surgical planning. JPS 2018;53:90-95
- Halleran DR, et al. Measure twice and cut once: Comparing endoscopy and 3D cloacagram for the common channel and urethral measurements in patients with cloacal malformations. JPS 2020;55:257-260
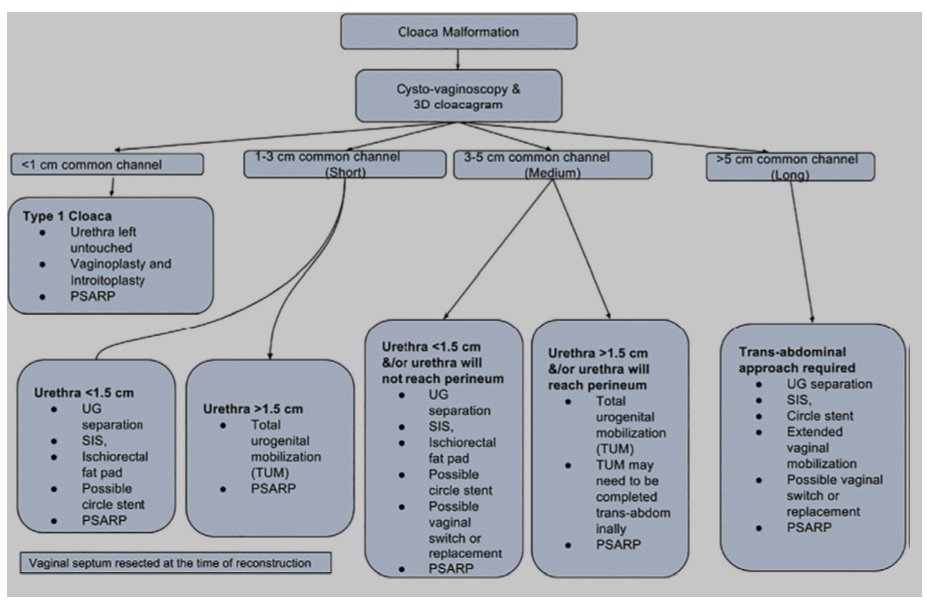 Source: Wood R, et al. Journal of Pediatric Surgery 2018;53:90-95
Source: Wood R, et al. Journal of Pediatric Surgery 2018;53:90-95
- Inflammatory bowel disease
- The nature of childhood IBD being more aggressive and requiring more surgery than the adult counterpart was well presented through the Helsinki and London experiences.
- The Helsinki series of IPAA with mean 10 years long term follow-up (n=80) showed overall surgical complication (53%) consisting mostly of adhesional bowel obstruction in half. Pouch failure of 10% with almost all related to late diagnosis of Crohn’s. Pouchitis is very common (73%). The group’s result can be found in Nyholm L, et al. JCC 2019;13:302-308
- Perianal Crohn’s disease (pCD) were discussed. Experience from Chelsea (n=18) with the use of seton for drainage, showed simple (66%) and complicated (33%) fistula had distinct difference in late recurrence of perianal sepsis after 6 months (8% vs. 100%), proposing a strong multidisciplinary approach to negate the need for ileostomy. This contrasted with the Toronto experience (n=57) of 23% ileostomy (Seemann et al. JPS 2015). Experience from Helsinki (n=13) following median 2-year follow-up showed 70% were symptom-free. Data in children based on use of biologics for pCD is based on the use of adalimumab (IMAgINE1 2012 and IMAgINE 2 2017) showed fistula closure at week 12, and maintained by 2 years.
 12th European Colorectal and Pelvic Reconstruction Conference, Vienna, Dec 2019
12th European Colorectal and Pelvic Reconstruction Conference, Vienna, Dec 2019
This year’s focus was on Urological and Colorectal care in anorectal malformation, but also included some topics related to Hirschsprung’s, acquired anorectal conditions, bowel/bladder management and transition care. There is a fantastic resource website with file sharing that you can download many of the presentations https://www.colorectal-vienna.com/file-share. An element of education was built in to the programme with The Medical University of Vienna put up a realistic cloacoscopy model for all attendees to practise; and a silicon perineal fistula model (from Nijmegen) was used for the practical workshop.
Mr Yew-Wei Tan
Evelina Children’s Hospital, London
[curated by Mark Davenport March 2020]